
Ketamine Infusion as an Adjunct in the Management of Sickle Cell Pain Crisis in a Pediatric Patient: A Case Discussion
By Piotr Kostyk, MD; David Shiovitz MD, PhD; Nitin Sekhri, MD
Department of Anesthesia
Westchester Medical Center
New York Medical College
New York, New York
INTRODUCTION
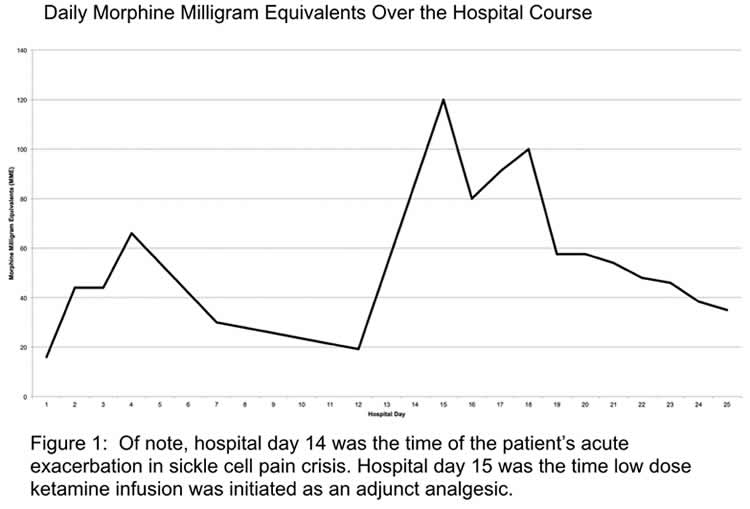
We present the case of a 10-year-old male with a history of sickle cell anemia who was admitted for sickle cell pain crisis initially controlled with an opioid regimen. However, during his hospital course, the patient suffered from an acute exacerbation in his pain crisis with escalations in his opioid and adjunct analgesic requirements with side effects from each noted, such as delirium and increased work of breathing. A low dose ketamine infusion was initiated, lessening the patient’s other analgesic medication requirements, as well as providing adequate analgesia as he recovered from his sickling pain crisis.
HOSPITAL COURSE
- Hospital day 1: Patient presented accompanied by mother complaining of pain primarily in his lower back, thighs, and knees. This was consistent with prior sickle cell pain crises. Initial analgesic regimen consisted of morphine PO PRN, acetaminophen IV, and ketorolac IV.
- Hospital day 2: Patient with uncontrolled pain. Morphine PCA initiated with PCA boluses for breakthrough pain.
- Hospital day 3: Patient opioid requirements were noted to be 44mg morphine through the PCA over the previous 24 hours. Regimen switched to hydromorphone PCA with PCA boluses.
- Hospital day 14: Patient requiring increasing amounts of hydromorphone via PCA over the previous hospital days. Noted to have acute exacerbation of pain in his bilateral knees (right greater than left) later this day, uncontrolled with hydromorphone PCA, and adjunct treatments (acetaminophen IV, ibuprofen PO, lidocaine patches). Overnight, the patient was transferred to the PICU for respiratory monitoring given rapid escalation of analgesics. Once there, he received midazolam, additional doses of ketorolac, and he was placed on a fentanyl infusion. At this time, the patient was febrile, WBC were markedly increased, an ultrasound of the right knee was concerning for a periosteal fluid collection, and blood cultures had grown coagulase negative Gram positive cocci. Broad spectrum antibiotics were initiated by the primary team.
- Hospital day 15: Patient noted to be delirious and with occasional clonic movements of his extremities, possibly related to opioid induced neurotoxicity. Fentanyl infusion was replaced with dexmedetomidine. The patient’s hydromorphone PCA was adjusted then, given his mental status changed to an authorized agent controlled analgesia (AACA) with a basal infusion. Low dose ketamine infusion was initiated and then titrated.
- Hospital day 23: In the prior days, patient pain control had improved, and he was able to ambulate. Delirium and clonic movements of the extremities had resolved. Opioid requirements decreased markedly. The hydromorphone boluses via AACA was discontinued, and the basal opioid, dexmedetomidine and ketamine infusions were weaned off. The patient ’s febrile episodes resolved, WBC returned to baseline, subsequent blood cultures were negative, and right knee pain and clinical findings were deemed to be due to avascular necrosis of the distal right femur. The patient was discharged home with analgesic regimen consisting of PO morphine and ibuprofen.
DISCUSSION
In the homozygous form of sickle cell disease, various triggers, such as hypoxia, dehydration, stress, and infections, trigger polymerization of hemoglobin. This causes sickling of erythrocytes, increased adhesion of these cells with the endothelium, causing small vessel occlusion and resultant local hypoxia and inflammation. Classically, pain management has centered on the early use of parenteral opioids, usually morphine, with escalation to intravenous opioid analgesia, and ultimately PCA pump for patients ’ with persistent pain. However, escalating opioid analgesic therapy also comes with higher likelihood of side effects, such as confusion, drowsiness, slowed breathing progressing to apnea, and constipation. Furthermore, chronic opioid exposure in this patient population may play a role in the development of refractory pain, which is thought to occur via activation of the NMDA receptor in the CNS, and the potentiation of nociceptive C fibers resulting in hyperalgesia and opioid tolerance. Ketamine is a non-competitive NMDA receptor antagonist that modulates opioid induced hyperalgesia and opioid tolerance. Additionally, this medication exhibits anti-inflammatory properties and has a wide therapeutic window. The use of ketamine in the setting of sickle cell pain crises has been limited to small retrospective case series as an adjunct to opioid therapy. Thus far, studies have shown that patients suffering from sickle cell pain crisis experience lower reported pain scores, reduced opioid-opioid-induced adverse effects, and decreased opioid dosing requirements when treated with ketamine infusion as an adjunct analgesic therapy.
CONCLUSIONS
Sickle cell pain crises are a debilitating consequence of sickle cell disease requiring prompt assessment and initiation of analgesia, with opioids being the mainstay of therapy. However, in this patient population, opioid-induced hyperalgesia and tolerance may develop from repeated pain management with these medications, possibly leading to escalating dose requirements and higher rates of adverse effects. Small studies have begun to show the benefits of ketamine as an adjunct to opioids in the management of sickle cell pain crises. In this patient with sickle cell pain refractory to opioids, low dose ketamine infusion was successful in decreasing opioid requirements and improving the patient ’s acute pain.
REFERENCES
- Ballas, S. K., Gupta, K., & Adams-Graves, P. (2012). Sickle cell pain: A critical reappraisal. Blood, 120(18), 3647-3656. https://doi.org/10.1182/blood-2012-04-383430.
- Lubega, F. A., DeSilva, M. S., Munube, D., Nkwine, R., Tumukunde, J., Agaba, P. K., Nabukenya, M. T., Bulamba, F., & Luggya, T. S. (2018). Low dose ketamine versus morphine for acute severe vaso occlusive pain in children: A randomized controlled trial. Scandinavian Journal of Pain, 18(1), 19-27. https://doi.org/10.1515/ sjpain-2017-0140.
- Palm, N., Floroff, C., Hassig, T. B., Boylan, A., & Kanter, J. (2018). Low-dose ketamine infusion for adjunct management during vaso-occlusive episodes in adults with sickle cell disease: A case series. Journal of Pain & Palliative Care Pharmacotherapy, 32(1), 20-26. https://doi.org/10.1080/15360288.2018.1468383
![]()



