Clinical Hypnosis in Pain & Symptom Management in Children
 By Haleh Saadat, MD
By Haleh Saadat, MD
Nationwide Children’s Hospital, Columbus, OH
The ability of the brain and body to adapt to acute and chronic stress is an increasingly important topic in scientific literature. The brain has an enormous impact on an individual’s physical and mental wellbeing by constantly sorting out information and engaging the neuroendocrine, autonomic and immune systems.1-2 Neuroscience is beginning to recognize the potential of brain plasticity after the early developmental period.
Chronic psychosocial stress and consequent physiological reaction can affect the individual’s wellbeing. Children are especially vulnerable to the negative effects of pain and anxiety. Pain in children is a multidimensional experience, which varies significantly based on child’s previous experience, personality, expectations and cognitive maturation.3,4 Psychological factors, such as anticipation and context have shown to be as important as the intensity of the stimulus in the experience of pain.5 Children often consider painful procedures to be the most difficult part of their illness. Neuroimaging studies have shown that the mere anticipation of a painful stimulus, in spite of the absence of direct physical stimulus, can activate various areas of the brain.6-8 It has been shown that it is the individual differences in the brain’s perception of the stressors that determines the body’s reactions, and in due course determines the vulnerability or resilience toward stress-related disorders.9-11
A multidisciplinary team approach in the treatment of pain that links the expertise and knowledge of several specialists (Pediatricians, Anesthesiologists, Psychologists, Nurses, child life specialists, etc.,) allows the development of an individual treatment plan and integration of the conventional medical interventions with the complementary approaches.
Hypnosis is one of the several methods that as an adjunct is considered to be effective in the management of variety of pain and other medical conditions. The American Psychological Association’s Division of Psychological Hypnosis defines hypnosis as a “therapeutic procedure in which a health professional makes suggestions that will help a patient experience post-hypnotic alterations in perception, sensation, emotion, thought, and/or behavior”.12
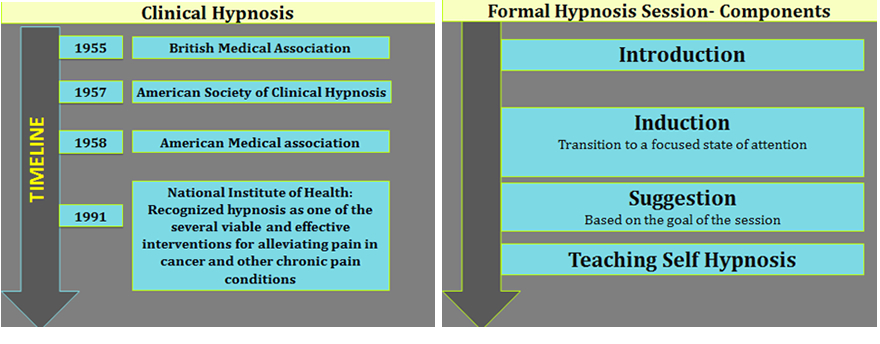
Hypnosis dates back several thousand years to the Greeks, Egyptians, and Persians. Dr. Milton Erickson and Dr. Ernest Hilgard were among the first investigators to utilize hypnosis in the United States. In 1958, The American Medical Association acknowledged hypnosis as a valuable tool in medical treatment.13 The National Institutes of Health Technology Assessment Panel recognized hypnosis as “a viable and effective intervention for alleviating pain with cancer and other chronic pain”, in 1996.14
Over the past few decades, hypnosis has been utilized in children undergoing painful medical treatments in the emergency room, during invasive diagnostic procedures such as bone marrow aspiration and lumbar puncture, and for the management of preoperative anxiety and post-operative pain. It has been used to treat pain associated with variety of chronic disorders, such as cancer, asthma, rheumatoid arthritis, migraine headache, cystic fibrosis, sickle cell disease, and burns.15-26 Several studies have also shown improvement with use of hypnosis in children and adolescents who suffered from behavioral conditions such as enuresis, and dysphasia, Tourette syndrome, trichotillomania, thumb-sucking, and dysphasia.27-32 The advancement of brain imaging techniques has shown that hypnosis can effectively alter or modify several aspects of the person’s psychological, physiological and neurological function.33-38 In addition, these imaging techniques have revealed that the modulation of pain by hypnosis is different from relaxation, cognitive coping, or a placebo-like mechanism.39
Hypnosis can be easily integrated in routine pediatric practice.40 Children’s vivid imaginations, their desire to learn, and the ease with which they intertwine fantasy and reality makes them great subjects for the use of hypnosis.41-42 A typical hypnosis session in adults and adolescents consists of induction, deepening of the trance state, delivery of specific suggestions and finally re-emergence. The induction phase helps focus the patient’s attention. The length and the manner that one achieves this phase in children varies according to the nature of the problem, the child’s developmental age, learning style, interests and strengths. Children respond to a large variety of hypnotic induction techniques. These methods and strategies include eye fixation and guided imagery, visual images of a favorite place, auditory images of a favorite song or movement images such as a flying blanket or sport activity. Additional techniques include story telling, idiomotor activities such as arm levitation and progressive muscle relaxation. Teaching self-hypnosis is the crucial part of the session. Encouraging the child to practice the learned skill is fundamental to a successful outcome because it would give them a sense of control and mastery. Parental cooperation, and that of the pain management team, are essential in achieving success.
The National Pediatric Hypnosis Training Institute (NPHTI)43 is the organization that provides education and skill development in clinical hypnosis and hypnotherapy for health care professionals who work in pediatric settings. They offer workshops in introductory, intermediate, and advanced pediatric hypnosis.
In summary, hypnosis is a reliable method as an adjunct to the conventional medicine in the management of acute, chronic, procedural pain as well as many other conditions in some children. Further evidence-based trials needed to address issues related to the optimal timing and length of hypnotic interventions.
References:
- Doidge, N. (2007) The brain that changes itself: stories of personal triumph from the frontiers of brain science, Penguin Books
- McEwen, B.S. and Gianaros, P.J. (2010) Central role of the brain in stress and adaptation: links to socioeconomic status, health, and disease. Ann. N. Y. Acad. Sci. 1186, 190–222
- McGrath PA: Aspects of pain in children and adolescents. J Child Psychol sychiatry. 1995;36:717-731.
- Ross DM, Ross SA. Childhood pain: Current issues, research and management. Baltimore: Urban & Schwartzenberg; 1988.
Chen, L.M. Imaging of Pain. (2007). International Anesthesiology Clinics. 44, 39-57. - Broome, M.E, Bates, T.A, Lillis, P.P, McGahee, T.W.(1990). Children's medical fears, coping behaviors, and pain perceptions during a lumbar puncture. ONF 17, 361-367.
- Price D.D. (2002). Central Neural Mechanisms that Interrelate Sensory and Affective Dimensions of Pain. Molecu Interven, 2:392-403.
- Porro C.A, Baraldi P, Pagnoni G. (2002). Does anticipation of pain affect cortical nociceptive systems? J Neurosci,. 22, 3206–3214.
- Hsieh J.C, Stone-Elander S, Ingvar M. (1999). Anticipatory coping of pain expressed in the human anterior cingulate cortex: a positron emission tomography study. Neurosci Lett. 262, 61–64.
- Lupien, S.J., McEwen, B.S., Gunnar, M.R., Heim, C., 2009. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat. Rev. Neurosci. 10, 434
- McEwen, B.S., 2009. The brain is the central organ of stress and adaptation. Neuroimage 47, 911
- Juster, R.-P., et al., Allostatic load biomarkers of chronic stress and impact on health and cognition. Neurosci. Biobehav. Rev. (2009)
- Rhue, J. W., Lynn, S. J., & Kirsch, I. (Eds.). (1993). Introduction to clinical hypnosis. In: Handbook of Clinical Hypnosis. Washington, DC: American Psychological Association.
- Council on Mental Health. Medical use of hypnosis. JAMA.1958:186 –189
- Integration of behavioral and relaxation approaches into the treatment of chronic pain and insomnia. NIH Technology Assessment Panel on Integration of Behavioral and Relaxation Approaches Into the Treatment of Chronic Pain and Insomnia. JAMA.1996;276:313–318
Martin-Herz S.P. Thurber C.A. Patterson D.R. (1986). Psychological principles of burn wound pain in children. II: Treatment applications. Journal Article. Research Support, U.S. Gov't, P.H.S. J Burn Care Rehab. 21, 458-72. - Iserson K.V. (1998). Hypnosis for pediatric fracture reduction. J Emerg Med 17, 53–56.
- Humphreys P, Gevirtz RN. (2000).Treatment of recurrent abdominal pain: components analysis of four treatment protocols. J Pediatr Gastroenterol Nutr 31, 47–51.
- Olness K, MacDonald J.T, Uden D.L. (1987). Comparison of self-hypnosis and propranolol in the treatment of juvenile classic migraine. Pediatrics 79, 593–597.
- Zeltzer L, LeBaron S. Hypnosis and nonhypnotic techniques for reduction of pain and anxiety during painful procedures in children and adolescents with cancer. J Pediatr, 1982; 101(6): 1032–5.
- Richter I.L, McGrath P.J, Humphreys P.J. (1986). Cognitive and relaxation treatment of paediatric migraine. Pain, 25, 195–203.
- Dinges, D.F, Whitehouse, W.G, Orne, E.C, Bloom, P.B, Carlin, M.M, Bauer, N.K, Gillen, K.A, Shapiro, B.S, Ohene-Frempong, K, Dampier, C, Orne, MT, (1997). Self-hypnosis training as an adjunctive treatment in the management of pain associated with sickle cell disease. Clinical Trial. Comparative Study. Internat J Clin Experim Hypn. 45, 417-432.
- Uman, L.S; Chambers, C.T; McGrath, P.J; Kisely, S. (2007). Psychological interventions for needle-related procedural pain and distress in children and adolescents. The Cochrane Database of Systematic Reviews, The Cochrane Library, The Cochrane Collaboration
- Genuis M.L. (1995). The use of hypnosis in helping cancer patients control anxiety, pain, and emesis: a review of recent empirical studies. Am J Clin Hypn 37, 316-325.
- Kohen DP. Hypnotherapeutic management of pediatric and adolescent trichotillomania. J Dev Behav Pediatr. 1996;17:328 –334 21.
- Kohen DP. Applications of relaxation and mental imagery (self-hypnosis) for habit problems. Pediatr Ann. 1991;20: 136–138, 141–144 22.
- Anbar RD. Self-hypnosis for management of chronic dyspnea in pediatric patients. Pediatrics. 2001;107(2).
- Culbert TP, Kajander RL, Kohen DP, Reaney JB. Hypnobehavioral approaches for school-age children with dysphagia and food aversion: a case series. J Dev Behav Pediatr. 1996;17: 335–341
- Kohen DP, Botts P. Relaxation-imagery (self-hypnosis) in Tourette syndrome: experience with four children. Am J Clin Hypn. 1987;29:227–237 24.
- Kohen DP, Mahowald MW, Rosen GM. Sleep-terror disorder in children: the role of self-hypnosis in management. Am J Clin Hypn. 1992;34:233–244
- Butler, L.D, Symons, B.K, Henderson, S.L. Shortliffe, L.D. Spiegel, D. (2005). Hypnosis reduces distress and duration of an invasive medical procedure for children. Clinical Trial. Journal Article. Randomized Controlled Trial. Research Support, Non-U.S. Gov't. Pediatrics. 115, e77-85.
- Huth M.M, Broome M.E, Good M. (2004). Imagery reduces children’s postoperative pain. Pain 110, 439–48.
- Lambert SA. (1996). The effects of hypnosis/guided imagery on the postoperative course of children. J Dev Behav Pediatr 17, 307–10.
- Zeltzer LK, Dolgin MJ, LeBaron S, LeBaron C. A randomized, controlled study of behavioral intervention for chemotherapy distress in children with cancer Pediatrics, 1991; 88(1): 34–42.
Rainville P, Duncan G.H. , Price D.D. (1997). Pain Affect Encoded in Human Anterior Cingulate But Not Somatosensory Cortex. Science, 277:5328; 968 – 971. - Rainville P, Hofbauer R.K, Bushnell, M.C, Duncan G.H, Price DD. (2000). Hypnosis modulates the activity in cerebral structures involved in arousal and attention. Poster presented at: Cognitive Neuroscience Society; San Francisco, CA.
- Rainville P , Hofbauer R.K, Bushnell M.C, Duncan G.H., Price D.D. (2002). Hypnosis Modulates Activity in Brain Structures Involved in the Regulation of Consciousness J Cognit Neurosci. 14, 887-901.
- Crawford, H.J, Horton, J.E, Harrington, G.S, Hirsch Downs, T, Fox, K, Daugherty, S, Downs, H III. (2000). Attention and dis-attention (hypnotic analgesia) to noxious somatosensory TENS stimuli: fMRI differences in low and highly hypnotizable individuals. Poster presented at: Sixth Annual Meeting of the Organization for Human Brain Mapping. San Antonio, TX.
- De Pascalis, V.F.S, Chiaradia, C, Carotenuto, E. (2002). The contribution of suggestibility and expectation to placebo analgesia phenomenon in an experimental setting. Pain, 3, 393-402.
- Chaves J.F., Dworkin, S.F. (1997), Hypnotic control of pain: Historical perspectives and future prospects. Internat J Clin Experim Hypn. 45:4:356-376.
- Chaves J.F., Dworkin, S.F. (1997), Hypnotic control of pain: Historical perspectives and future prospects. Internat J Clin Experim Hypn. 45:4:356-376.
- Faymonville M.E, Mambourg P.H, Joris J, et al. (1997) Psychological approaches during conscious sedation: hypnosis versus stress reducing strategies: a prospective randomized study. Pain 73, 361-367.
- Olness K, Kohen D.P. (1996). Hypnotic induction for children, techniques, strategies and approaches. Hypnosis and Hypnotherapy with Children 5, 52-87
Olness K, Gardner G.G. (1978). Some Guidelines for Uses of Hypnotherapy in Pediatrics. Pediatrics 62, 228-233. - Olness K, Kohen D.P. (1996). Correlates of childhood hypnotic responsiveness. Hypnosis and Hypnotherapy with Children. 4, 33-52.
- Sugarman LI. Hypnosis: teaching children self-regulation. Pe- diatr Rev. 1996;17:5–11
- http://www.nphti.net/ Accessed on January 24, 2015.