Complementary Medical Therapies for Pain Management
Massage Therapy in Pediatric Pain Management
By Mary C. McLellan, MPH, BSN, RN, CMT
Integrative Therapies Team
Boston Children’s Hospital
Boston, MA
Massage therapy is defined as the “systematic and scientific manipulation of the soft tissues of the body”1. Soft tissue includes muscles, lymphatic and circulatory vessels, connective tissue and fascia. There are many styles, approaches and applications of massage therapy (See Table 1) but they all have five basic techniques to treat the body:
- Effleurage – long, broad strokes which stimulate the parasympathetic response and passively stretches broad muscle groups
- Petrissage – kneading and compression to relax and stretch muscles and connective tissue
- Friction – deep pressure applied to the muscles and connective tissues in a cross-fiber direction
- Tapotement – percussion techniques to relax spastic muscles
- Vibration – gentle, rhythmic movement of large muscle groups to induce a parasympathetic response
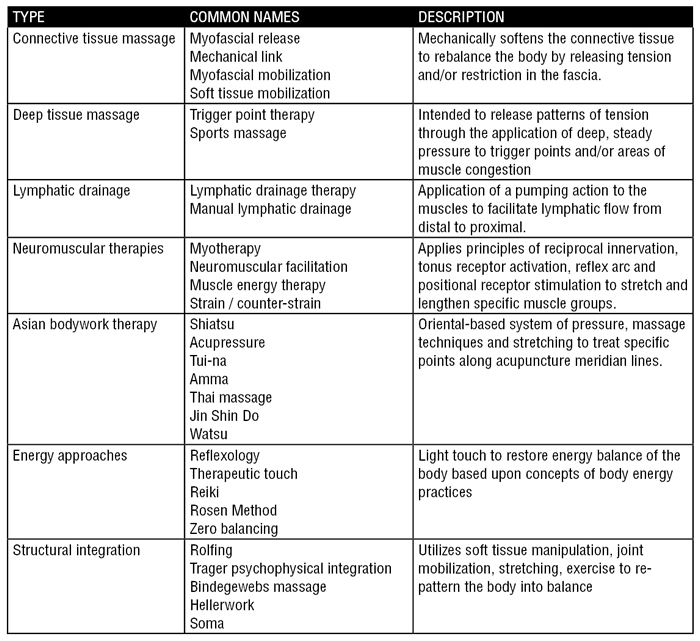
Table 1
The massage therapist integrates these techniques based upon the treatment needs, massage modality and the patient’s goals.
There are many therapeutic effects of massage therapy in relation to pain management and pain reduction. Following the Gate Control theory, pressure applied to trigger points may override transmission of pain stimuli along the large diameter nerve fibers 2–4. The mechanical effects of massage may warm and stretch the soft tissues, decrease fibrous adhesions, and activate either the parasympathetic or sympathetic system (dependent upon massage approach) which may influence muscle tone. Utilizing massage therapy prior to physical therapy (PT) is a helpful adjunct to improve comfort of the patient and prepare the tissues for PT interventions5,6. Controlled studies have demonstrated massage to be more effective than relaxation techniques for reducing musculoskeletal pain7–9. Studies have demonstrated massage therapy to be effective in reducing reported pain6,7,16–25,8,26,27,9–15, post-operative analgesic usage21,28–30, cancer related pain and symptoms10,11,31,12,13,16–19,22,24, chronic pain9,32, back pain and related disability6,8,23,25,26,33,34, tension headaches7, and other musculoskeletal pain4,7–9,18,25,26.
Massage should not be performed over areas of skin or tissue integrity loss, acute injury or inflammation, pitting edema, or locations that have indwelling devices such as central venous lines or shunts. Massage should not be done in the setting of circulatory disorders that are associated with increased thrombus risk such as varicosities, phlebitis, and/or thrombophlebitis. Massage should be deferred if the patient has an active infectious condition that could be spread along the skin, the circulation or lymphatic system. Caution should be observed in areas with abnormal or absent skin sensation as the sensory feedback of the applied massage pressure and put the patient at risk for injury. Caution should be used in patients with prolonged bleeding times from either anti-coagulation, low platelets (<50,000K) or coagulopathies.
To date, 45 states have licensure for massage therapists; however, the training qualifications and requirements vary greatly. The American Massage Therapy Association (AMTA) is a professional organization of massage therapists that pledge to uphold a Code of Ethics and professional standards35. AMTA members must have completed at least 500 in-class hours from an accredited massage therapy school, state licensure or certification from the National Certification Board for Therapeutic Massage and Bodywork (NCBTMB). The AMTA has a free “Find a Therapist” feature on their website which is available to the public. The NCBTMB provides national certification for professional massage therapists and bodyworkers for professionals that have graduated from a NCBTMB assigned school. Therapists obtain CBTMB certification after passing a NCBTMB board certification exam, pass a NCMTMN-run criminal background check, have state licensure and agree to uphold to the NCBTMB Standards of Practice and Code of Ethics36,37. Professionals must reapply every two years after completing 24 continuing education credits. The NCBTMB has a free provider search for the public to find a qualified therapist. Similar to the AMTA, the American Organization for Bodywork Therapies of Asia (AOBTA) is a professional organization for therapists trained in Asian Bodywork Therapies (ABT) that have completed 500 hours of AOBTA training38. The AOBTA has a free search for the public to find an ABT therapist. Patients may look for therapists with membership or credentialing from any of the mentioned professional organizations to ensure they are receiving treatment from a professionally trained and qualified massage therapist.
Massage is an effective therapy for a variety of pain conditions and should be considered for inclusion in a patient’s pain management plan.
References
- Tappan F. Healing Massage Techniques: Holistic, Classic and Emerging Methods. (Lange A&, ed.). Norwalk, CT; 1988.
- Katz J, Rosenbloom B. The golden anniversary of Melzack and Wall’s gate control theory of pain: Celebrating 50 years of pain research and management. Pain Res Manag. 2015;20(6):285–286.
- Fritz S. Mosby’s Fundamentals of Therapeutic Massage. St. Louis, MO: Mosby Lifeline; 1995.
- Simons D, Simons L, Travel J. Travell and Simons’ Myofascial Pain and Dysfunction: The Trigger Point Manual (2 Volumes) Edition. Baltimore, MD: Lippincott Williams and Williams.; 1998.
- Fiechter J, Brodeur R. Manual and manipulation techniques for rheumatic disease. Med Clin North Am. 2002;86:91-103.
- Preyde M. Effectiveness of massage therapy for subacute low-back pain: a randomized control trial. CMAJ. 2002;162:1815-1829.
- Quinn C, Chandler C, Moraska A. Massage therapy and frequency of chronic tension headaches. Am J Public Health. 2002;92:1657-1661.
- Hernandez-Reif M, Field T, Krasnegor J, Theakston H. Lower back pain is reduced, and range of motion increased after massage therapy. Int J Neurosci. 2001;106:131-145.
- Hasson D, Arnetz B, Jelveus L, Edelstam B. A randomized clinical trial of the treatment effects of massage compared to relaxation tape recordings on diffuse long-term pain. Psychother Psychosom. 2004;73:17-24.
- Toth M, Marcantonio ER, Davis RB, Walton T, Kahn JR, Phillips RS. Massage Therapy for Patients with Metastatic Cancer: A Pilot Randomized Controlled Trial. J Altern Complement Med. 2013;19(7):650-656. doi:10.1089/acm.2012.0466.
- Da Cunha Batalha LM, Mota AASC. Massage in children with cancer: Effectiveness of a protocol. J Pediatr. 2013;89(6):595-600. doi:10.1016/j.jped.2013.03.022.
- Mehling W, Jacobs B, Acree M, et al. Symptom management with massage and acupuncture in postoperative cancer patients: a randomized control trial. J pain symptom Manag. 2007;33:258-266.
- Cassileth B, Vickers A. Massage therapy for symptoms control: outcome study at a major cancer center. J pain symptom Manag. 2004;28(3).
- Field T, Hernandez-Reif M, Seligman S, et al. Juvenille rheumatoid arthritis benefits from massage therapy. J Pediatr Psychol. 1997;22:607-617.
- Moyer C, Rounds J, Hannum J. A meta-analysis of massage therapy research. Psychol Bull. 2004;130:3-18.
- Post-White J, Kinney M, Savik K, Gau J, Wilcox C, Lerner I. Therapeutic massage and health touch improves symptoms in cancer. Integr Cancer Ther. 2003;2:332-344.
- Smith M, Reeder F, Daniel L, Baramee J, Hagman J. Outcomes of touch therapies during bone marrow transplantation. Altern Ther Heal Med. 2003;9:40-49.
- Smith M, Kemp J, Hemphil L, Vojir C. Outcomes of therapeutic massage for hospitalized cancer patients. J Nurs Scholarsh. 2002;34:257-262.
- Weinrich S, Weinrich M. The effect of massage on pain in cancer patients. Appl Nurs Res. 1990;3:140-145.
- Tsao J. Effectiveness of massage therapy for chronic, non-malignant pain: a review. Evidence-based Complement Altern Med. 2007:4165–79.
- van der Dolder P, Roberts D. A trial into the effectiveness of soft tissue massage in the treatment of shoulder pain. Aust J Physiother. 2003;49(3):183-188.
- Grealish L, Lomansney A, Whiteman B. Foot massage; a nursing internvention to modify the distressing symptoms of pain and nausea in patients hospitalized with cancer. Cancer Nurs. 2000;23:237-243.
- Furlan A, Brosseau L, Imamura M, Irvin E. Massage for low back pain: a systematic review within the framework of the Cochrane Collaboration Back Review Group. Spine (Phila Pa 1976). 2002;27:1896-1910.
- Ferrell-Tory A, Glick O. The use of therapeutic massage as a nursing intervention to modify anxiety and the perception of cancer pain. Cancer Nurs. 1993;16(93-101).
- Cherkin D, Sherman K, Deyo R, Shekelle P. A review of the evidence for the effectiveness, safety, and cost of acupuncture, massage therapy and spinal manipulation for back pain. Ann Intern Med. 2003;138:898-906.
- Cherkin D, Eisenberg D, Sherman K, et al. Randomized trial comparing traditional Chinese medical acupuncture, therapeutic massage and self-care education for chronic low back pain. Arch Intern Med. 2001;161:1081-1088.
- Adams R, White B, Beckett C. The effects of massage therapy on pain management in the acute care setting. Int J Ther Massage Bodyw Res Educ Pract. 2010;3(1):4-11.
- Piotrwoski M, Paterson C, Mitchinson A, Kim H, Kirsh M, Hinshaw D. Massage as adjunctive therapy in the management of acute postoperative pain: a preliminary study in men. J Am Coll Surg. 2003;197(6):1037-1046.
- Taylor A, Galpner D, Taylor P, et al. Effects of adjunctive Swedish massage and vibration therapy on short-term postoperative outcomes: a randomized, controlled trial. J Altern Complement Med. 2003;9:77-89.
- LeBlanc-Lourvry I, Costaglioli B, Boulon C, Leroi A, Ducrotte P. Does mechanical massage of the abdominal wall after colectomy reduce postoperative pain and shorten the duration of an ileus? J Gastrointest Surg. 2002;6(1):43-49.
- Karagozoglu S, Kahve E. Effects of back massage on chemotherapy-related fatigue and anxiety: Supportive care and therapeutic touch in cancer nursing. Appl Nurs Res. 2013;26(4):210-217. doi:10.1016/j.apnr.2013.07.002.
- Castro-Sánchez AM, Matarán-Pearrocha GA, Granero-Molina J, Aguilera-Manrique G, Quesada-Rubio JM, Moreno-Lorenzo C. Benefits of massage-myofascial release therapy on pain, anxiety, quality of sleep, depression, and quality of life in patients with fibromyalgia. Evidence-based Complement Altern Med. 2011;2011. doi:10.1155/2011/561753.
- Cherkin DC, Sherman KJ, Kahn J, et al. A comparison of the effects of 2 types of massage and usual care on chronic low back pain: A randomized, controlled trial. Ann Intern Med. 2011;155(1):1-9. doi:10.7326/0003-4819-155-1-201107050-00002.
- Hsieh LLC, Kuo CH, Lee LH, Yen AMF, Chien KL, Chen THH. Treatment of low back pain by acupressure and physical therapy: Randomised controlled trial. Br Med J. 2006;332(7543):696-698. doi:10.1136/bmj.38744.672616.AE.
- American Massage Therapy Association. Code of Ethics. https://www.amtamassage.org/About-AMTA/Core-Documents/Code-of-Ethics.html. Accessed May 24, 2019.
- NCBTMB. Board certification requirements. https://www.ncbtmb.org/certificants/. Accessed May 24, 2019.
- NCBTMB. NCMBTM Code of Ethics. https://www.ncbtmb.org/code-of-ethics/. Published 2017. Accessed May 24, 2019.
- AOBTA. Asian Bodywork Therapies definition, scope and profession. https://aobta.org/page/Def_Scope_Profession. Accessed May 24, 2019.